Scientists now know how long it takes for a cell to tell itself it’s time to die.
Signals triggering a type of cell suicide called apoptosis move through a cell like a wave, traveling at a rate of 30 micrometers per minute, Stanford University systems biologists Xianrui Cheng and James Ferrell Jr. report in the Aug. 10 Science.
These findings resolve a debate over whether these death signals spread by diffusion, with signaling molecules working their own way across a cell, or as self-regenerating trigger waves, like toppling dominoes. The apoptosis process starts with damage that causes the release of death signal chemicals. One example is cytochrome c leaking from damaged mitochondria, the cell’s power plant. Once cytochrome c concentrations get high enough, the chemicals signal proteins called caspases to go to work. Caspases trigger other proteins to poke holes in neighboring mitochondria, releasing more cytochrome c and moving the death wave across the cell. That chain reaction happens more quickly than diffusion can, Ferrell says. In an African clawed frog egg, a trigger wave takes about a half-hour to spread across the 1.2 millimeter cell, whereas diffusion would take five hours, he says.
Like forest fires, trigger waves will keep going as long as there is fuel to feed them — in this case, the death signal chemicals and proteins, Ferrell says. He predicts that many other biological signals may move as trigger waves.
“We biologists are just waking to this idea that trigger waves are a recurring theme in biological communication,” Ferrell says.
Discovering that apoptosis travels as trigger waves in cells may give scientists clues about how to persuade cancer cells to kill themselves (SN: 1/21/17, p. 10). Or researchers may learn how to prevent cells from dying in conditions such as Alzheimer’s disease or muscular dystrophy.
Pregnant women aren’t immune to the escalating opioid epidemic.
Data on hospital deliveries in 28 U.S. states shows the rate of opioid use among pregnant women has quadrupled, from 1.5 per 1,000 women in 1999 to 6.5 per 1,000 women in 2014, the U.S. Centers for Disease Control and Prevention reports.
The highest increases in opioid use among pregnant women were in Maine, New Mexico, Vermont and West Virginia, according to the CDC study, published online August 9 in Morbidity and Mortality Weekly Report. “This analysis is a stark reminder that the U.S. opioid crisis is taking a tremendous toll on families,” says coauthor Jean Ko, a CDC epidemiologist in Atlanta.
In this first look at opioid use during pregnancy by state, Washington, D.C. had the lowest rate in 2014, at 0.7 per 1,000 women, and Vermont had the highest, at 48.6 per 1,000. However, the data from the U.S. Health and Human Services Department represents only the 28 states that record opioid use at childbirth during the studied time frame.
“We knew the incidence was increasing” as the number of babies going through opioid withdrawal has also gone up, says Matthew Grossman, a pediatrician at Yale University. Overall, the number of U.S. deaths attributed to opioids has also been steadily rising (SN: 3/31/18, p. 18). In 2014, there were 14.7 opioid deaths per 100,000 people, up from 6.2 per 100,000 in 2000, according to the CDC. Taking opioids during pregnancy, especially in the last trimester, increases the risk of preterm birth and stillbirth, as well as infant opioid withdrawal (SN: 6/10/17, p. 16). Pregnant women should tell their doctors if they are taking opioids, so complications can be addressed, says Alison Holmes, a pediatrician at Dartmouth-Hitchcock Medical Center in Lebanon, N.H. Mothers may be prescribed methadone, a synthetic opioid which is safer for the fetus and protects it from going through withdrawal in the womb. “What’s not safe for the child is active opioid misuse,” she says.
Only eight U.S. states require that pregnant women be tested for opioids if substance abuse is suspected, the CDC says. In Cincinnati, all pregnant women are tested at delivery, but it would be even better to test women in the first trimester, says pediatrician Scott Wexelblatt at the Cincinnati Children’s Hospital. “If we could identify a mom at 12 weeks instead of 40 weeks, then we could get her into medicated assisted treatment.”
In one published swoop, an ancient fossil fruit bat has turned into a lemur. If that transformation holds, it suggests that lemur ancestors made two tricky sea crossings from Africa to Madagascar, not one as researchers have often assumed.
A new fossil analysis finds that the ancient species Propotto leakeyi, which lived in East Africa between 23 million and 16 million years ago, was not a bat, as scientists thought, but a primate closely related to modern aye-ayes. These strange-looking lemurs are found only on Madagascar along with another closely related lemur lineage. What’s more, Propotto teeth and jaws display key similarities with fossils of a roughly 34-million-year-old primate, Plesiopithecus teras, previously found in Egypt, researchers say. Plesiopithecus, previously suspected to have been a primate, was an ancestor of Propotto and of modern aye-ayes, they conclude. Together, the findings, published August 21 in Nature Communications, may help rewrite lemurs’ evolutionary history.
The research challenges a long-standing view that all Madagascar lemurs, including aye-ayes, evolved from a single population of African ancestors that somehow reached the island at least 54 million years ago. That estimate rests largely on genetic studies of modern lemurs and other primates. Destruction of ancient lemurs’ African habitats by global cooling around 34 million years ago left their kind isolated on Madagascar, according to this scenario.
But the survival of aye-aye ancestors in Africa millions of years after that, as suggested in the new study, raises the possibility that Propotto reached Madagascar on its own — separate from the other lemur lineage found on the island — and gave rise to present-day aye-ayes. No Propotto fossils have been found on Madagascar.
“Our identification of both Propotto and Plesiopithecus as African relatives of the aye-aye implies that [these] lemurs weren’t present on Madagascar until 30 million years or more later than previously thought,” says study coauthor paleontologist Erik Seiffert of the University of Southern California in Los Angeles. Ancestors of the modern lemurs other than aye-ayes traveled to Madagascar sometime between around 41 million and 20 million years ago, the researchers estimate. During that period, ancestors of the only other mammal groups now inhabiting Madagascar — rodents, Malagasy mongooses and insect-eating creatures called tenrecs — also reached the island from Africa. Previous computer simulations indicated that ocean currents at that time could have carried animals stranded on storm-uprooted trees and vegetation mats from East Africa to Madagascar.
The team, which included Duke University’s Gregg Gunnell (who died in 2017), created digital reconstructions of Plesiopithecus and Propotto fossils for comparison with fossil and living primates, including aye-ayes (Daubentonia), and to closely related mammals called colugos. Evolutionary trees based on tooth and jaw analyses and available DNA data pointed to a link between the two ancient species and aye-ayes.
Plesiopithecus and Propotto might have used enlarged teeth projecting from the front of their mouths to gouge holes in trees and expose grubs’ nests, as modern aye-ayes do. Aye-ayes also poke through tree holes with long, skinny middle fingers to extract grub. But no hand fossils from either ancient creature have been found, so it’s a mystery whether they shared aye-ayes’ taste for finger food.
The discoverer of three Propotto tooth-bearing lower jaws in Kenya originally reported in 1967 that the finds belonged to a new primate species, possibly an ancestor of primate relatives of lemurs called lorises. But within the next two years, the same scientist accepted another researcher’s proposal that Propotto’s jaws and teeth more closely resembled those of a fruit bat. A 1984 report describing several more Propotto teeth unearthed in Kenya also concluded that they came from a fruit bat.
The new identification of a line of ancient African lemurs that ran from Plesiopithecus through Propotto “is an interesting discovery,” says paleoanthropologist Marc Godinot of the National Museum of Natural History in Paris. “I have thought for years that Propotto was more likely a primate than a fruit bat.”
Godinot also argued in a 2006 study that the shape and positioning of teeth at the front of Plesiopithecus’ mouth pegged it as a relative of aye-ayes, consistent with a double colonization of Madagascar by lemur ancestors.
That possibility “merits serious consideration,” but a single African origin for lemurs on Madagascar remains the simplest, most likely scenario, says evolutionary biologist Anne Yoder of Duke University. Most African mammals couldn’t manage even one colonization of the island, so attributing two of these “highly improbable” events to lemur ancestors alone demands more evidence, Yoder says.
Still, it can’t be discounted that several ancient African lines of primates might have evolved in the aye-aye lineage but only one made it to Madagascar on a sea crossing that occurred independently of other African lemurs, Yoder says. Or, in line with her own view, Madagascar may have been colonized by one group of ancient lemurs that gave rise to multiple lines of creatures, one of which was a direct ancestor of modern aye-ayes. Only further fossil discoveries can resolve this mystery, Yoder says.
For cervical cancer screening, there’s a new option in town.
Women ages 30 to 65 can opt to have human papillomavirus, or HPV, testing alone every five years, according to new recommendations from the U.S. Preventive Services Task Force.
HPV testing alone joins two other alternatives that are still endorsed: an HPV test plus a Pap test every five years, or a Pap test alone every three years. The guidelines, published online August 21 in JAMA, are the first update to the group’s cervical cancer screening recommendations since 2012.
Recent research has shown that HPV testing, which checks for the presence of the sexually transmitted virus in a sample of cervical cells, is better at catching precancerous lesions early than the traditional Pap test, which looks for those lesions in a cervical cell sample.
Globally, cervical cancer is the fourth most common cancer among women. HPV causes nearly all cervical cancers.
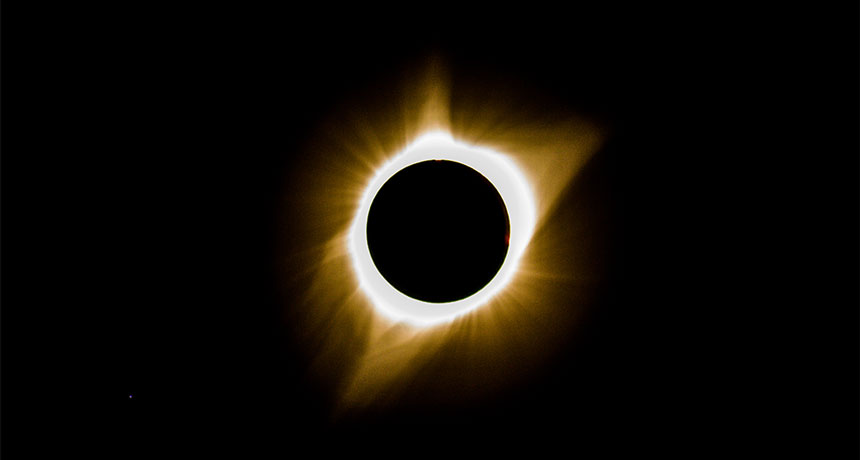
It’s been a year since the total solar eclipse of August 21, 2017, captured millions of imaginations as the moon briefly blotted out the sun and cast a shadow that crisscrossed the United States from Oregon to South Carolina.
“It was an epic event by all measures,” NASA astrophysicist Madhulika Guhathakurta told a meeting of the American Geophysical Union in New Orleans in December. One survey reports that 88 percent of adults in the United States — some 216 million people — viewed the eclipse either directly or electronically. Among those were scientists and citizen scientists who turned their telescopes skyward to tackle some big scientific mysteries, solar and otherwise. Last year, Science News dove deep into the questions scientists hoped to answer using the eclipse. One year out, what have we learned?
The eclipse sent ripples through Earth’s atmosphere. Normally, the sun’s radiation splits electrons from atoms in the atmosphere, forming a charged layer called the ionosphere, which stretches from 75 to 1,000 kilometers up. But when sunlight briefly disappears during an eclipse, the electrons rejoin their atoms, creating a disturbance in the ionosphere that is detectable with receivers on the ground (SN Online: 8/13/17).
The moon’s supersonic shadow produced a bow wave of atoms piling up in the ionosphere, similar to the wave at the prow of a boat, Shun-Rong Zhang of MIT’s Haystack Observatory in Westford, Mass., reported in December. Although such bow waves were predicted in the 1960s, this was the first time they were definitively observed. The eclipse also sent a wave traveling through the thermosphere, an uncharged layer of the atmosphere about 250 kilometers high, that was observed from as far away as Brazil nearly an hour after the eclipse ended (SN: 5/26/18, p. 14). And measurements of temperature, wind speed and sunlight intensity showed that the eclipse briefly changed the weather along the path of darkness.
Showing Einstein was right is not so simple. Physicists chased the moon’s shadow to redo the iconic experiment that showed Einstein’s theory of general relativity was correct (SN Online: 8/15/17). In Einstein’s view, the sun’s mass should warp spacetime enough that the positions of stars should appear to be slightly different during an eclipse. During the May 1919 solar eclipse, British astronomer Arthur Stanley Eddington took photographs that proved Einstein right.
During the 2017 eclipse, almost a century later, amateur astronomer Donald Bruns of San Diego made similar measurements with modern equipment and came to the same conclusion as Eddington: Stars visible during the eclipse were all askew. Bruns published his results in Classical and Quantum Gravity in March.
But astrophysicist Bradley Schaefer of Louisiana State University in Baton Rouge and others had far more difficulty reproducing the measurement with enough precision to show that Einstein was right. “‘Bummer’ is an understatement,” Schaefer says. “This all may have been for naught.”
Schaefer had enough trouble that he thinks it may have been impossible for Eddington to get the precision he claimed. The earlier astronomer may have hit upon the right answer by luck, not because he actually measured it.
Infrared light will help measure the corona’s magnetic field. Some eclipse experiments didn’t revolutionize our understanding of the sun on their own, but will enable future ones to pull back the veil. One of these was the first infrared observations of the sun’s corona, the shimmering halo of hot, diffuse plasma that is only visible in its entirety during a total solar eclipse. The shape and motion of all that plasma are guided by magnetic fields, but the corona’s magnetic field is so weak that it has never been measured directly (SN Online: 8/16/17). Previous studies suggested that infrared wavelengths of light might be particularly sensitive to the corona’s magnetic field. So two groups chased the August 2017 eclipse in airplanes to get some infrared observations. Amir Caspi of the Southwest Research Institute in Boulder, Colo., and his colleagues took the first infrared image of the entire corona. Flying in another aircraft, Jenna Samra of Harvard University measured the corona in five specific wavelengths, one of which had never been seen before. Comparing those results with observations taken from the ground in Casper, Wyo., (where I watched the eclipse) showed that those wavelengths are bright enough that a telescope now under construction in Hawaii will be able to help map the corona’s magnetism (SN Online: 5/29/18).
Figuring out what heats the corona will take more work. Almost every experiment aimed at the eclipsed sun last August had some bearing on the biggest solar mystery of all: Why is the corona so hot? The solar surface simmers at around 5500° Celsius, but the corona — despite being farther away from the solar furnace and made of much more diffuse material — rages at millions of degrees.
One year after the Great American Eclipse, scientists are still scratching their heads. Caspi’s team searched for waves rippling through the corona, which could distribute energy far from the solar surface. Those waves could also help comb out magnetic tangles in the corona and explain its well-ordered look (SN Online: 8/17/17).
In a complementary measurement, the group in Wyoming saw signs of neutral helium atoms in the corona, says solar physicist Philip Judge of the National Center for Atmospheric Research in Boulder. Those uncharged atoms probably represent cool material embedded in the corona (SN Online: 6/16/17).
Similar cool spots have been seen during earlier eclipses, although it’s hard to imagine how the cool atoms survive in the searing heat, like ice cubes remaining solid in hot soup. But collisions between charged ions and neutral atoms could help convert ordered motions, like Caspi’s waves, into coronal heat.
The results so far are interesting, but inconclusive, Caspi says. “It’s certainly possible we will get some very interesting results from this set of observations alone,” he says. But for such a big problem as coronal heating, eclipse observations may play a supporting role to more direct measurements, such as those that the recently launched Parker Solar Probe will make (SN Online: 8/12/18).
People are already looking to the next eclipse. A survey done by researchers at the University of Michigan found that eclipse watchers sought more information about eclipses and the scientific questions involved an average of 16 times in the three months following the event.
Several research groups are planning observations for the next total eclipses, visible in South America in July 2019 and December 2020 (SN: 8/5/17, p. 32). Caspi and Samra’s teams both hope to fly through those eclipses in aircraft again.
And amateurs and pros alike are preparing for the Great American Eclipse version 2.0, which will cross from Texas to Maine in 2024.
Particle accelerator technology has crested a new wave.
For the first time, scientists have shown that electrons can gain energy by surfing waves kicked up by protons shot through plasma. In the future, the technique might help produce electron beams at higher energies than currently possible, in order to investigate the inner workings of subatomic particles.
Standard particle accelerators rely on radiofrequency cavities, metallic chambers that create oscillating electromagnetic fields to push particles along. With the plasma wave demonstration, “we’re trying to develop a new kind of accelerator technology,” says physicist Allen Caldwell of the Max Planck Institute for Physics in Munich. Caldwell is a spokesperson of the AWAKE collaboration, which reported the results August 29 in Nature. In an experiment at the particle physics lab CERN in Geneva, the researchers sent beams of high-energy protons through a plasma, a state of matter in which electrons and positively charged atoms called ions comingle. The protons set the plasma’s electrons jiggling, creating waves that accelerated additional electrons injected into the plasma. In the study, the injected electrons reached energies of up to 2 billion electron volts over a distance of 10 meters.
“It’s a beautiful result and an important first step,” says Mark Hogan, a physicist at SLAC National Accelerator Laboratory in Menlo Park, Calif., who studies plasma wave accelerators.
Previously, scientists have demonstrated the potential of plasma accelerators by speeding up electrons using waves set off by a laser or by another beam of electrons, instead of protons (SN: 5/8/10, p. 28). But proton beams can carry more energy than laser or electron beams, so electrons accelerated by protons’ plasma waves may be able to reach higher energies in a single burst of acceleration. The new result, however, doesn’t yet match the energies produced in previous plasma accelerators. Instead, the study is just a first step, a proof of principle that shows that proton beams can be used in plasma wave accelerators.
High-energy electrons are particularly useful for particle physics because they are elementary particles — they have no smaller constituents. Protons, on the other hand, are made up of a sea of quarks, resulting in messier collisions. And because each quark carries a small part of the proton’s total energy, only a fraction of that energy goes into a collision. Electrons, however, put all their oomph into each smashup.
But electrons are hard to accelerate directly: If put in an accelerator ring, they rapidly bleed off energy as they circle, unlike protons. So AWAKE starts with accelerated protons, using them to get electrons up to speed.
Prior to the experiment, there was skepticism over whether the plasma could be controlled well enough for an effort like AWAKE to work, says physicist Wim Leemans of Lawrence Berkeley National Laboratory in California, who works on laser plasma accelerators. “This is very rewarding to see that, yes, the plasma technology has advanced.”
We now have the most precise estimates for the strength of gravity yet.
Two experiments measuring the tiny gravitational attraction between objects in a lab have measured Newton’s gravitational constant, or Big G, with an uncertainty of only about 0.00116 percent. Until now, the smallest margin of uncertainty for any G measurement has been 0.00137 percent.
The new set of G values, reported in the Aug. 30 Nature, is not the final word on G. The two values disagree slightly, and they don’t explain why previous G-measuring experiments have produced such a wide spread of estimates (SN Online: 4/30/15). Still, researchers may be able to use the new values, along with other estimates of G, to discover why measurements for this key fundamental constant are so finicky — and perhaps pin down the strength of gravity once and for all. The exact value of G, which relates mass and distance to the force of gravity in Newton’s law of universal gravitation, has eluded scientists for centuries. That’s because the gravitational attraction between a pair of objects in a lab experiment is extremely small and susceptible to the gravitational influence of other nearby objects, often leaving researchers with high uncertainty about their measurements. The current accepted value for G, based on measurements from the last 40 years, is 6.67408 × 10−11 meters cubed per kilogram per square second. That figure is saddled with an uncertainty of 0.0047 percent, making it thousands of times more imprecise than other fundamental constants — unchanging, universal values such as the charge of an electron or the speed of light (SN: 11/12/16, p. 24). The cloud of uncertainty surrounding G limits how well researchers can determine the masses of celestial objects and the values of other constants that are based on G (SN: 4/23/11, p. 28). Physicist Shan-Qing Yang of Huazhong University of Science and Technology in Wuhan, China, and colleagues measured G using two instruments called torsion pendulums. Each device contains a metal-coated silica plate suspended by a thin wire and surrounded by steel spheres. The gravitational attraction between the plate and the spheres causes the plate to rotate on the wire toward the spheres.
But the two torsion pendulums had slightly differently setups to accommodate two ways of measuring G. With one torsion pendulum, the researchers measured G by monitoring the twist of the wire as the plate angled itself toward the spheres. The other torsion pendulum was rigged so that the metal plate dangled from a turntable, which spun to prevent the wire from twisting. With that torsion pendulum, the researchers measured G by tracking the turntable’s rotation.
To make their measurements as precise as possible, the researchers corrected for a long list of tiny disturbances, from slight variations in the density of materials used to make the torsion pendulums to seismic vibrations from earthquakes across the globe. “It’s amazing how much work went into this,” says Stephan Schlamminger, a physicist at the National Institute of Standards and Technology in Gaithersburg, Md., whose commentary on the study appears in the same issue of Nature. Conducting such a painstaking set of experiments “is like a piece of art.”
These torsion pendulum experiments yielded G values of 6.674184 × 10−11 and 6.674484 × 10−11 meters cubed per kilogram per square second, both with an uncertainty of about 0.00116 percent.
This record precision is “a fantastic accomplishment,” says Clive Speake, a physicist at the University of Birmingham in England not involved in the work, but the true value of G “is still a mystery.” Repeating these and other past experiments to identify previously unknown sources of uncertainty, or designing new G–measuring techniques, may help reveal why estimates for this key fundamental constant continue to disagree, he says.
Now that heart recipients can realistically look forward to leaving the hospital and taking up a semblance of normal life, the question arises, what kind of semblance, and for how long? South Africa’s Dr. Christiaan Barnard, performer of the first heart transplant, has a sobering view…. “A transplanted heart will last only five years — if we’re lucky.” — Science News, September 14, 1968
Update Barnard didn’t need to be so disheartening. Advances in drugs that suppress the immune system and keep blood pressure down have helped to pump up life expectancy after a heart transplant. Now, more than half of patients who receive a donated ticker are alive 10 years later. A 2015 study found 21 percent of recipients still alive 20 years post-transplant. In 2017, nearly 7,000 people across 46 countries got a new heart, according to the Global Observatory on Donation and Transplantation.
New images of gas churning inside an ancient starburst galaxy help explain why this galactic firecracker underwent such frenzied star formation.
Using the Atacama Large Millimeter/submillimeter Array, or ALMA, researchers have taken the most detailed views of the disk of star-forming gas that permeated the galaxy COSMOS-AzTEC-1, which dates back to when the universe was less than 2 billion years old. The telescope observations, reported online August 29 in Nature, reveal an enormous reservoir of molecular gas that was highly susceptible to collapsing and forging new stars. COSMOS-AzTEC-1 and its starburst contemporaries have long puzzled astronomers, because these galaxies cranked out new stars about 1,000 times as fast as the Milky Way does. According to standard theories of cosmology, galaxies shouldn’t have grown up fast enough to be such prolific star-formers so soon after the Big Bang.
Inside a normal galaxy, the outward pressure of radiation from stars helps counteract the inward pull of gas’s gravity, which pumps the brakes on star formation. But in COSMOS-AzTEC-1, the gas’s gravity was so intense that it overpowered the feeble radiation pressure from stars, leading to runaway star formation. The new ALMA pictures unveil two especially large clouds of collapsing gas in the disk, which were major hubs of star formation. “It’s like a giant fuel depot that built up right after the Big Bang … and we’re catching it right in the process of the whole thing lighting up,” says study coauthor Min Yun, an astronomer at the University of Massachusetts Amherst.
Yun and colleagues still don’t know how COSMOS-AzTEC-1 stocked up such a massive supply of star-forming material. But future observations of the galaxy and its ilk using ALMA or the James Webb Space Telescope, set to launch in 2021, may help clarify the origins of these ancient cosmic monsters (SN Online: 6/11/14).
One fine Hawaiian day in 2015, Geoff Zahn and Anthony Amend set off on an eight-hour hike. They climbed a jungle mountain on the island of Oahu, swatting mosquitoes and skirting wallows of wild pigs. The two headed to the site where a patch of critically endangered Phyllostegia kaalaensis had been planted a few months earlier. What they found was dispiriting.
“All the plants were gone,” recalls Zahn, then a postdoctoral fellow at the University of Hawaii at Manoa. The two ecologists found only the red flags placed at the site of each planting, plus a few dead stalks. “It was just like a graveyard,” Zahn says.
The plants, members of the mint family but without the menthol aroma, had most likely died of powdery mildew caused by Neoerysiphe galeopsidis. Today the white-flowered plants, native to Oahu, survive only in two government-managed greenhouses on the island. Why P. kaalaensis is nearly extinct is unclear, though both habitat loss and powdery mildew are potential explanations. The fuzzy fungal disease attacks the plants in greenhouses, and the researchers presume it has killed all the plants they’ve attempted to reintroduce to the wild.
Zahn had never encountered extinction (or near to it) so directly before. He returned home overwhelmed and determined to help the little mint. Just like humans and other animals, plants have their own microbiomes, the bacteria, fungi and other microorganisms living on and in the plants. Some, like the mildew, attack; others are beneficial. A single leaf hosts millions of microbes, sometimes hundreds of different types. The ones living within the plant’s tissues are called endophytes. Plants acquire many of these microbes from the soil and air; some are passed from generation to generation through seeds.
The friendly microbes assist with growth and photosynthesis or help plants survive in the face of drought and other stressors. Some protect plants from disease or from plant-munching animals. Scientists like Zahn are investigating how these supportive communities might help endangered plants in the wild, like the mint on the mountain, or improve output of crops ranging from breadbasket wheat to tropical cacao.
Beyond the garden store Certain microbial plant partners are well-known, and there are scores of microbial products already on the market. Gardeners, for instance, can spike their watering pails with microbes to encourage flowering and boost plant immunity. But “we know very little about how the products out there actually do work,” says Jeff Dangl, a geneticist at the University of North Carolina at Chapel Hill. “None of those garden supply store products have proven useful at large scale.”
Big farms can use microbial treatments. The main one applied broadly in large-scale agriculture helps roots collect nitrogen, Dangl says, which plants use to produce chlorophyll for photosynthesis.
Farmers may soon have many more microbial helpers to choose from. Scientists studying plant microbiomes have described numerous unfamiliar plant partners in recent decades. Those researchers say they’ve only scratched the surface of possibilities. Many start-up companies are researching and releasing novel microbial treatments. “The last five years have seen an explosion in this,” says Dangl, who cofounded AgBiome, which soon plans to market a bacterial treatment that combats fungal diseases. Agricultural giants like Bayer AG, which recently bought Monsanto, are also investing hundreds of millions of dollars in potential microbial treatments for plants.
The hope is that microbes can provide the next great revolution in agriculture — a revolution that’s sorely needed. With the human population predicted to skyrocket from today’s 7.6 billion to nearly 10 billion by 2050, our need for plant-based food, fibers and animal feed is expected to double.
“We’re going to need to increase yield,” says Posy Busby, an ecologist at Oregon State University in Corvallis. “If we can manage and manipulate microbiomes … this could potentially represent an untapped area for increasing plant yield in agricultural settings.” Meanwhile, scientists like Zahn are eyeing the microbiome to save endangered plants.
But before microbiome-based farming and conservation can truly take off, many questions need answers. Several revolve around the complex interactions between plants, their diverse microbial denizens and the environments they live in. One concern is that the microbes that help some plants might, under certain conditions, harm others elsewhere, warns microbiologist Luis Mejía of the Institute of Scientific Research and High Technology Services in Panama City.
Save the chocolate Cacao crops — and thus humankind’s precious M&M’s supply — are under constant threat from undesirable fungi, such as Phytophthora palmivora, which causes black pod rot. But there are good guys in cacao’s microbiome too, particularly the fungus Colletotrichum tropicale, which seems to protect the trees. Natalie Christian, as a graduate student at Indiana University Bloomington, traveled to the Smithsonian Tropical Research Institute on Panama’s Barro Colorado Island in 2014 to study how entire communities of microbes colonize and influence cacao plants (Theobroma cacao). Christian suspected that the prime source of a young cacao tree’s microbiome would be the dead and decaying leaves on the rainforest or orchard floor.
To test this hunch and see what kind of protection microbes picked up from leaf litter might offer, Christian raised fungus-free cacao seedlings in a lab incubator. When the plants reached about half a meter tall, she placed them in pots outside, surrounding some with leaf litter from a healthy cacao tree, some with litter from other kinds of trees and some with no litter at all.
After two weeks, she brought the plants back into the greenhouse to analyze their microbiomes. She found nearly 300 kinds of endophytes, which she, Mejía and colleagues reported last year in Proceedings of the Royal Society B.
The microbiome membership differed between the litter treatments. Plants in pots with either kind of leaf litter possessed less diverse microbiomes than those without litter, probably because the microbes in the litter quickly took over before stray microbes from elsewhere could settle in. These results suggest that a seedling in the shadow of more mature trees will probably accumulate the same microbiome as its towering neighbors. To see if some of those transferred microbes protect the cacao from disease-causing organisms, Christian rubbed a bit of black pod rot on the leaves of plants in each group. Three weeks later, she measured the size of the rotted spots.
Plants surrounded by cacao litter had the smallest lesions. Those with litter from other trees had slightly more damage, and plants with no litter had about double the damage of the mixed litter plants.
“Getting exposed to the litter of their mother or their own kind had a very strong beneficial effect on the resistance of these young plants,” says plant biologist Keith Clay of Tulane University in New Orleans, a coauthor of the study.
Scientists aren’t sure how the good fungi protect the plants against the rot. It may be that the beneficial fungi simply take up space in or on the leaves, leaving no room for the undesirables, Christian says. Or a protective microbe like C. tropicale might attack a pathogen via some kind of chemical warfare. In the case of cacao, she thinks the most likely explanation is that the good guys act as a sort of vaccine, priming the plant’s immune system to fight off the rot. In support of this idea, Mejía reported in 2014 in Frontiers in Microbiology that C. tropicale causes cacao to turn on defensive genes.
Cacao farmers may need to rethink their practices. The farmers normally clear leaf litter out of orchards to avoid transmitting disease-causing microbes from decaying leaves to living trees, says Christian, now a postdoc at the University of Illinois at Urbana-Champaign. But her work suggests that farmers might do well to at least hold on to litter from healthy trees.
Crop questions Litter is a low-tech way to spread entire communities of microbes — good and bad. But agricultural companies want to grab only the good microbes and apply them to crops. The hunt for the good guys starts with a stroll through a crop field, says Barry Goldman, vice president and head of discovery at Indigo Ag in Boston. Chances are, you’ll find bigger and hardier plants among the crowd. Within those top performers, Indigo has found endophytes that improve plant vigor and size, and others that protect against drought.
The company, working with cotton, corn, rice, soybeans and wheat, coats seeds with these microbes. Once the seeds germinate, the microbes cover the newborn leaves and can get inside via cuts in the roots or through stomata, tiny breathing holes in the leaves. The process is akin to what happens when a baby travels through the birth canal, picking up beneficial microbial partners from mom along the way. For example, the first-generation Indigo Wheat, released in 2016, starts from seeds treated with a beneficial microbe. In Kansas test fields, the treatment raised yields by 8 to 19 percent.
Farmers are also reporting improved drought tolerance. During the first six months of 2018 with only two rains, the participating Kansas farmers had given up on and plowed over fields with struggling regular wheat, but not those growing Indigo Wheat, Goldman says.
In St. Louis, NewLeaf Symbiotics is interested in bacteria of the genus Methylobacterium. These microbes, found in all plants, are known as methylotrophs because they eat methanol, which plants release as their cells grow. In return for methanol, M-trophs, as NewLeaf calls them, offer plants diverse benefits. Some deliver molecules that encourage plants to grow; others make seeds germinate earlier and more consistently, or protect against problem fungi.
NewLeaf released its first products this year, including Terrasym 401, a seed treatment for soybeans. Across four years of field trials, Terrasym 401 raised yields by more than two bushels per acre, says NewLeaf cofounder and CEO Tom Laurita. One bushel is worth about $9. On farms with thousands of acres, that adds up.
Farmers are pleased, but NewLeaf’s and Indigo’s work is hardly done. Plant microbiome companies all face similar challenges. One is the diverse environments where crops are grown. Just because Indigo Wheat thrives in Kansas doesn’t mean it will outgrow standard varieties in, say, North Dakota. “The big ask for the next-gen ag biotech companies like AgBiome or Indigo … is whether the products will deliver as advertised over a range of field conditions,” Dangl says.
Another issue is that crop fields and plants already have microbiomes. “We’re asking a lot of a microbe, or a mix of microbes, to invade an already-existing ecosystem and persist there and do their job,” Dangl says. Companies will need to make sure their preferred microbes take hold.
And while scientists are well aware that diverse microbial communities cooperate to affect plant health, most companies are working with one kind of microbe at a time. Indigo isn’t yet sure how to approach entire microbiomes, Goldman says, but “we certainly are thinking hard about it.”
Researchers are beginning to address these questions by studying microbes in communities — such as Christian’s leaf-litter microbiomes — instead of as individuals. In the lab, Dangl developed a synthetic community of 188 root microbes. He can apply them to plants under stress from drought or heat, then watch how the communities respond and affect the plants.
A major aim is to identify the factors that determine microbiome membership. What decides who gets a spot on a given plant? How does the plant species and its local environment affect the microbiome? How do plants welcome friendlies and eject hostiles? “This is a huge area of importance,” Dangl says.
There’s some risk in adding microbes to crops while these questions are still unanswered, Mejía cautions. Microbes that are beneficial in one situation could be harmful in other plants or different environments. It’s not a far-fetched scenario: There’s a fungal endophyte of a South American palm tree that staves off beetle infestations when the trees are in the shade. Under the sun, however, the fungus turns nasty, spewing hydrogen peroxide that kills plant tissues.
And although C. tropicale benefits cacao, the genus has a dark side: Many species of Colletotrichum can cause leaf lesions and rotted fruit or flower spots in a variety of plants ranging from avocados to zinnias. Microbes for conservation Back in Hawaii, after that disheartening hike to the P. kaalaensis graveyard, Zahn pondered how to protect native plants in wild environments such as Oahu’s mountains.
In people, Zahn considered, antibiotics can damage normal gut microbe populations, leaving a person vulnerable to infection by harmful microbes. P. kaalaensis got similar treatment in the greenhouse, where it received regular dosing of fungicide. In retrospect, Zahn realized, that treatment probably left the plants bereft of their natural microbiome and weakened their immune systems, leaving them vulnerable to mildew infection once dropped into the jungle.
For people on antibiotics, probiotics — beneficial bacteria — can help restore balance. Zahn thought a similar strategy, a sort of plant probiotic, could help protect P. kaalaensis in future attempts at moving it outside.
For a probiotic, Zahn looked to a P. kaalaensis cousin, Phyllostegia hirsuta, which can survive in the wild. He put P. hirsuta leaves in a blender and sprayed the slurry over P. kaalaensis growing in an incubator.
Then, Zahn placed a leaf infected with powdery mildew into the incubator’s air intake. The mint plants treated with the P. hirsuta slurry experienced delayed, less severe infections compared with untreated plants, Zahn and Amend, also at the University of Hawaii at Manoa, reported last year in PeerJ. The probiotic had worked.
Zahn used DNA sequencing to identify the microbes in the slurry. Many of the microbiome members probably benefit P. kaalaensis, but he thinks he’s found a major protector: a yeast called Pseudozyma aphidis that lives on leaves. “This yeast normally just passively absorbs nutrients from the environment,” Zahn says. “But given the right victim, it will turn into a vicious spaghetti monster.” When mildew spores land nearby, the yeast grows tentacle-like filaments that appear to envelop and feed on the mildew.
Emboldened by his results, Zahn trekked back to the jungle and planted six slurry-treated plants in April 2016. They survived for about two years, but by May 2018, they were all dead. “It was still a huge win,” says Nicole Hynson, a community ecologist also at Manoa. After all, P. kaalaensis without probiotics last only months. And the probiotics approach might apply beyond one little Hawaiian mint, Hynson adds: “We’re really at the beginning of thinking how we might use the microbiome to address plant restoration.”
Zahn has since moved to Utah Valley University in Orem, where he’s hoping to help endangered cacti with microbes. Meanwhile, he’s left the Phyllostegia project in the hands of Jerry Koko, a graduate student in Hynson’s lab. Koko is studying how the yeast and some root-based fungi protect the plant.
Hynson says their goal is to build “a superplant.” With probiotics on both roots and shoots, an enhanced P. kaalaensis should be well-equipped to grow strong and resist mildew. In greenhouse experiments so far, Koko says, the plants with both types of beneficial fungi seem to sport fewer, smaller powdery mildew patches than plants that received no probiotic treatment.
While the restoration of a little flowering plant, or a few more bushels of soybeans, may seem like small victories, they could herald big things for plant microbiomes in conservation as well as agriculture. The farmers and conservationists of the future may find themselves seeding and tending not just plants, but their microscopic helpers, too.